Common Challenges Faced by USA Thalidomide Survivors
 Imagine; you live in a body that resembles few others. Instead of 10 fingers, you have three. Instead of two legs, you have one and a half. Your congenital uniqueness doesn’t stop there. Your anatomy, arms, legs, toes, fingers, muscles, bones, blood vessels, and almost every bodily system entail structures which challenge society’s constructs of “normality”. Some people label you as “disabled”. Others perceive you as “courageous”. Still others see you as hopeless and helpless. You see yourself as different and yet ‘not different’.
Imagine; you live in a body that resembles few others. Instead of 10 fingers, you have three. Instead of two legs, you have one and a half. Your congenital uniqueness doesn’t stop there. Your anatomy, arms, legs, toes, fingers, muscles, bones, blood vessels, and almost every bodily system entail structures which challenge society’s constructs of “normality”. Some people label you as “disabled”. Others perceive you as “courageous”. Still others see you as hopeless and helpless. You see yourself as different and yet ‘not different’.
Historically, societies are never truly prepared to respond to (let alone understand) people born with rare physiological differences. Prescribed for morning sickness in the late 1950s and early 1960s, the drug ‘thalidomide’ caused tens of thousands of severe birth defects world-wide before being pulled from global markets, including the United States. No other group of individuals is drawn together based on the vast differences of their congenital anomalies. Such is the case with thalidomide survivors born in the United States.
Thalidomide’s Impact on Fetal Development
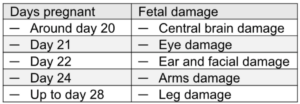
Here’s a brief explanation of how taking thalidomide during pregnancy interferes with fetal development.
Thalidomide interferes with the developing embryo by blocking the formation of blood vessels to inhibit limb and organ development leading to severe limb, ear, eye, heart, and kidney malformations and absences. The specific type of damage to fetal development depends on the time and duration of ingestion during the first month of pregnancy.
 While the damage to one’s body created by thalidomide can create an extensive range of life difficulties for thalidomide survivors, today we will look at a foundational issue: Thalidomide’s effect, and impact, on blood vessel development.
While the damage to one’s body created by thalidomide can create an extensive range of life difficulties for thalidomide survivors, today we will look at a foundational issue: Thalidomide’s effect, and impact, on blood vessel development.
1. Vein Access
Because thalidomide impedes blood vessel development in the developing fetus, a common trait shared by most thalidomide survivors is extremely limited access to veins for blood work and medical therapies like an IV.
Whether for acute or long-term medical care, IV access is essential for the: 1. Administration of fluids (including medication, replacement blood, or nutrients) intravenously, and/or 2. Measuring health status and the effectiveness of medical treatment through blood draws.
Most people have numerous “superficial veins” (veins that are close to the skin’s surface) in their hands, arms, feet and legs. However, due to poor blood vessel development, the “superficial veins” of thalidomide survivors’ are virtually non-existent. Therefore, phlebotomists (and medical staff who draw blood or insert an IV) must insert the IV needle more deeply and more often in several limbs as they search for what are called “deep veins”. The ‘deep veins’ thalidomide survivors are scarce, buried deeper in the dermis of the skin, and bruise or roll when needles attempt to penetrate them.
Further complicating vein access is the fact that most thalidomide survivors have aged to their late 50s and 60s. Survivors are at an age when vein access becomes even more difficult for nearly all older adults. This is primarily due to age-related changes that make veins fragile, less elastic, and harder to stabilize.
Here are a few thalidomide survivor stories regarding attempted IV access and blood draws.
a) I was on the operating table being prepped for a hip replacement. After 14 failed attempts to access a vein, I told the surgical team, “Get your best phlebotomist. I’m giving you one more chance. If you can’t find a vein, I’m cancelling this surgery.”
b) Finding a vein to access in my hands, arms, feet or legs is nearly impossible.
c) I was in my doctor’s office for a routine workup. After nine attempts to find a vein, they gave up trying.
d) I’ve been in the hospital twice in the past year. My hospital stay was uncharacteristically extended 3 to 4 days each time as they were unable to access a vein to draw blood to determine whether the treatment was effective.
e) I now experience trauma every time blood work is required or asked for. My veins are so deep medical staff have to really dig down deep to access a vein. In the meantime, their multiple attempts hurt like hell and those attempts usually end up bruising or scaring my limited vein access.
f) Throughout my life medical staff have only found two veins they can access. However, they are so close together that they usually prioritize only one for an IV, leaving no vein access for a blood draw.
g) Often insurance or medical services will not approve the installation of a vein port for medical or financial reasons.
To reduce the need for repeated needle sticks, installing a PICC line is a potential solution. A PICC line (Peripherally Inserted Central Catheter) is a long, thin, flexible tube inserted through a vein near the heart for long-term blood draws as well as the delivery of antibiotics, chemotherapy, or nutrition.
Having open access to a major vein for weeks or months at a time comes with risks including pain, bleeding, infection, thrombosis, or catheter dislodgement. A PICC line also requires routine flushing with saline to prevent blood clots, stop medication buildup, and to ensure the line remains functional. Due to risks, on-going maintenance, and cost of surgical installation clinicians and insurance are reticent to install a PICC line.
Utilization of IV therapy is a hospital care standard today. In fact, hospitalized patients receive Intravenous (IV) therapy 80–90% of the time during their stay. Regretfully, thalidomide survivors face the pain and discomfort of multiple needle sticks, ofttimes to no avail. Unfortunately, many healthcare providers still do not have the knowledge, protocols or equipment in place to care for a patient with very limited access to a vein.
Burt, age 1